It’s been a difficult year to be a biotech investor. The SPDR Biotech ETF (XBI) is down 17% YTD. Things started out harshly in January 2016 with a precipitous drop of 35%, and despite a nice recovery during the middle of the year, the past month has been rather unkind to investors. Yet, not all companies have struggled in 2016. Shares of CoLucid Pharmceuticals, Inc. (NASDAQ: CLCD) are up a whopping 290% YTD, thanks largely to the release of positive topline data from the company’s first Phase 3 trial with lasmiditan in September 2016.CLD
Lasmiditan is a first-in-class 5-HT1F receptor agonist currently in Phase 3 development for the treatment of acute migraine attack. The company reported positive topline data from the first Phase 3 trial in early September 2016. The data sent shares of CoLucid flying over 300% higher over the next week. The release of further data from that study and a strong institutional financing put the shares at nearly $40 earlier in October, up from below $5 back in February 2016.
The market value of CoLucid shares today is just below $600 million, and although this is a 5-fold increase from January 1st, I think there still may be significant upside left in the name. Below I attempt to address some of the key questions investors might have about the story.
– What is a migraine headache, anyway?
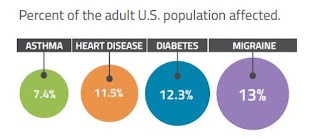
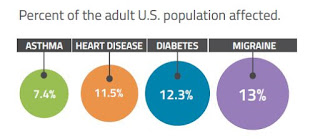
A migraine is a serious, debilitating neurological condition. The disease affects roughly 13% of the global population and is more common than asthma, heart disease, and diabetes in the U.S. (source: U.S. CDC, 2014). That equates to approximately 36 million individuals in the U.S., approximately 2% of which report having ? 15 or more episodes per month according to the 2011 Project Atlas study by the World Health Organization. Women affected outnumber men 4-to-1. In fact, migraines affect 30% of women over a lifetime and impacts life in almost 1 out of 4 households (source: American Headache Society).
– What causes a migraine?
Migraines are often idiopathic in nature but can be triggered by food, environmental factors, stress, weather, and exposure to light. There is even genetic predisposition to a migraine, with approximately 80% of migraine sufferers having a family history of a migraine affecting a first-degree relative (source: American Headache Society). Comorbidity with cardiovascular disease is also quite common, and patients with a migraine have a 54% increase in the risk of developing coronary artery disease (CAD) compared to the general population (9.9% vs. 6.4%) per IMS Health claims.
– Don’t most migraine patients just take OTC medications, like ibuprofen or naproxen?
According to data from IMS Health, sourced from adjudicated claims for health plan enrollees across the U.S., roughly 4 million adults in the U.S. are diagnosed with migraine headaches, which is only slightly above 10% of the total afflicted population based on the WHO Project Atlas study. That means nearly 32 million Americans either do not know they have migraines – presumably they just assume they get really bad tension headaches – or know but chose to manage their disease without pharmaceutical intervention.
Of diagnosed patients, approximately 50% attempt to manage the disease by the use of OTC medications, including non-steroidal anti-inflammatory drugs (ibuprofen, naproxen, etc…), aspirin, and acetaminophen. However, for many moderate-to-severe migraine sufferers, NSAIDs, and other OTC medications do not provide sufficient relief. Thus, these 2 million individuals each year will visit a primary care physician (65%), neurologist (20%), or headache specialist (15%) seeking prescription medications to treat their disease.
However, even prescription drugs do not work for the most severely impacted. IMS Health reports that over 5 million ER visits per year are due to migraines. The direct medical costs associated with migraines in the U.S. approximate $17 billion. Over 90% of individuals with migraines report missing work due to an attack, leading to 112 million days of lost work annually (IMS Health, 2016). Another 50% say that migraines restrict activities or interfere with daily activities on a regular basis (Migraine.com). Indirect medical costs from lost work or lost productivity amount to another $15 billion in the U.S.
So while OTC medications to treat a migraine are quite common, the are effective in less than half of the patients. And, as noted above, the increase in incidence of comorbid cardiovascular disease is concerning to migraine patients taking frequent NSAID. NSAIDs do increase the risk of cardiovascular events in at-risk patients.
– Most migraine patients are prescribed triptans, right? Why do we need another class of drugs when triptans work and are now super cheap (generic)?
Within the prescription market, triptans control the majority of the share, accounting for 91% of migraine prescriptions and 72% of migraine units according to a June 2010 audit by IMS Health. Sumatriptan, sold by GlaxoSmithKline (NYSE: GSK) as Imitrex® is the triptan market leader, with approximately 75% market share. Imitrex generated peak sales in the U.S. of approximately $1.1 billion before the patent expiration in 2008. Pharmacies dispensed approximately 13 million prescriptions for Triptan or Triptan-products during 2014. One-third of these patients are taking multiple drugs to control their disease. Migraine prescription drug sales in seven countries (U.S. and Europe) were estimated to be $3.3 billion in 2015 and are expected to grow to $4.4 billion in 2020.
So these are a very popular choice for prescription-seeking migraine sufferers; however, despite the popularity of triptans, approximately 76% of triptan users have conditions or risk factors as defined by the Framingham Heart Study results (2003) that contraindicate or warn against triptan use (IMS Health, 2016). These triptan-intolerable patients included those at high risk for coronary artery disease, a history of stroke, peripheral vascular disease and chronically uncontrolled high blood pressure. These patients are also often on concomitant medications that could have potentially dangerous side-effects when used in combinations with triptans.
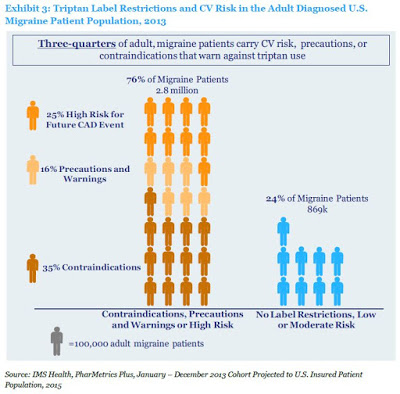
For example, the label for sumatriptan includes “Warnings and Precautions” that note potential risks for use of the drug in patients with a history of myocardial ischemia, myocardial infarction, and angina. Sumatriptan is contraindicated for use in these patients. The FDA also cautions on use of the drug in patients with a history of arrhythmias, chest, throat, neck, and/or jaw pain or pressure, or at risk for cerebrovascular events. Even worse, mixing a triptan with a NSAID like naproxen potentially creates even more risk. Below is a screenshot of the “Black Box” for Treximet®, a combination sumatriptan/naproxen tablet sold by Pernix Therapeutics (NASDAQ: PTX).











Leave A Comment