TM Editors Note: This article discusses a penny stock and/or microcap. Such stocks are easily manipulated; do your own careful due diligence.
Overview
This report is an extensive update on almost everything I know about the DCVax-L phase 3 trial and is over 20 pages long. The catalyst for this report was the recent information on the still blinded phase 3 trial presented in June at ASCO. It will take dedicated investors a great deal of time to read this report in its entirety. For a quick overview, the Key Points section summarizes my key conclusions and can be quickly read. The other parts will take more time and effort so that you may want to read just one of these sections at a time. Here is the organization of the report.
Key Points lists my most important conclusions and hypotheses.
New Information from ASCO
Encouraging Open Label data from the Information Arm of the Phase 3 Study and the Phase 1/2 Studies
Background Information for Help in Understanding the Phase 3 Trial
Thoughts on Potential FDA Interpretation of Phase 3 Trial
Examples of the Long Term Survival Tail for the Checkpoint Inhibitor Opdivo
Key Points
I continue to believe that the phase 3 trial of DCVax-L in newly diagnosed glioblastoma has a very good chance for success. The trial remains ongoing and blinded.
Key opinion leaders involved in the trial have stated that patients appear to be living much longer than would be expected if they were treated only with current standard of care.
The trial remains blinded but new information on the phase 3 trial presented at ASCO adds supports to the hypothesis that DCVax-L is providing an impressive survival benefit over and above standard of care.
This long term survival hypothesis is further reinforced by open label data which comes from two other data sets: (1) 25 patients treated in the information arm of the phase 3 trial and (2) 20 patients treated in the phase 1/2 trial. Both data sets showed impressive survival benefits as compared to standard of care and long term survival tails that compare favorably to those seen with checkpoint inhibitors.
Results from the two studies just cited suggest that with DCVax-L, the difference in the percentage of patients who remain alive for a long time period (say two or more years) as compared to the percentage of patients who remain alive on SOC at that same time point (the survival tail) is comparable to that seen with checkpoint inhibitors (Opdivo, Keytruda, Tecentriq) in other aggressive solid tumors such as advanced cases of non-small cell lung cancer and melanoma. It is the long term survival tail that has excited key opinion leaders about the checkpoint inhibitors.
The design of the phase 3 trial is such that patients whose cancers progress on standard of care are switched to DCVax-L. Also, patients who progress on DCVax-L remain on DCVax-L because trials with other immune therapies like the checkpoint inhibitors have shown survival benefits even after the cancer has progressed. This is all done in a blinded fashion.
The median time for progression for standard of care is about seven months so that many patients on SOC could have been quickly switched to DCVax-L. It was reported at ASCO that 90% of the patients in the trial were on DCVax-L. This is very close to being a blinded single arm study and could explain why patients appear to be living longer than would be expected with SOC.
We know that the trial was randomized 2:1 in favor of DCVax-L so that 67% or 221 of the 331 patients enrolled in trial revieved only DCVax-L. By simple arithmatic, we can calculate that 23% or 76 of the patients first received standard of care and were switched to DCVax-L and that 10% or 34 received only standard of care. This cross over design does not affect the statistical analysis of mPFS but it does require a special analysis for mOS which could create some ambiguity in ferreting out the effect of DCVax-L. I understand there is a statistical method for this type of analysis.
Because of this aspect of the trial, I think that the FDA may place great weight on the length of time that patients survive as compared to historical SOC results determined in other trials. This would be in addition to the analysis of the two primary but independent endpoints of mPFS and mOS.
One of the strong attributes of DCVax-L is its safety profile. The most frequent side effects are a fever after injection that can be treated with Tylenol and mild pain and irritation at the site of intradermal injection. Out of more than 2,000 intradermal injections given to over 400 patients, there have only been 7 patients who experienced serious adverse events that investigators deemed to be related or possibly related to the DCVax-L treatment. Five of these were seizures and it is important to note that because GBM is growing rapidly in the brain that the disease itself can cause seizures. Because safety can be as important to a drug as its efficacy, this is a major plus for DCVax-L.
The trial is likely to continue for an indeterminate time beyond July at which time one of the minimum stopping thresholds for the trial of 233 deaths is likely to be reached. This is because of a statistical technique called censoring. With censoring, all patients still alive in the trial would not be included in the analysis of mOS, one of the two primary endpoints in the trial. In the case of the DCVax-L trial, the 100 patients still alive would be dropped from the analysis and the calculation would be based on the 231 patients who have died. However, some of the patients who responded best to DCVax-L are likely to be included in this group of 100. Because of this, the Company has a compelling reason to let the trial run longer in order to to allow the data to mature further.
The FDA has shown much greater flexibility in approving new cancer drugs in the last few years. It has approved the checkpoint inhibitors Opdivo and Keytruda on the basis of small studies with end points of objective response or mPFS with no data on survival in some aggressive cancers. The data set for DCVax-L will be large and will have much data on survival. In the event of ambiguities in the two separate primary endpoints of mPFS and mOS, the long term survival that I am hypothesizing might be compared to historical SOC results and could be a key factor in the FDA’s decision on approval.
The Company is burning about $1.5 million per month. They are financing this burn by raising small amounts of capital that usually provide only a few months of cash. The goal is to minimize the amount of dilution until the topline results of the phase 3 trial are available. This could potentially involve one, two or more such small raises.
If my hypothesis about results in the phase 3 trial is correct, it should lead to approval. DCVax-L could be a major medical advance and commercial blockbuster, possibly comparable to the checkpoint inhibitors. I am obviously standing virtually alone in this opinion as evidenced by the $0.17 penny stock share price and micro-cap valuation of $33 million placed on the company. If my view were the consensus, the stock would likely have a market capitalization of $1 billion or more.
The trial remains ongoing and blinded. Neither the Company nor investigators will know how the results for DCVax-L added to SOC compares to SOC alone until the trial is ended; the data base is locked and scrubbed; and statistical analyses are performed. The arguments I present in this note are suggestive, but by no means conclusive evidence that the trial will be successful.
Acronyms Used Extensively in this Report
GBM: Glioblastoma multiforme is stage 4 brain cancer
SOC: The standard of care in newly diagnosed GBM patients is surgical resection followed by treatment with radiation and the chemotherapy drug temozolomide
PFS: Progression free survival is the time from when the surgery is performed until the tumor begins to regrow
mPFS: The time at which the cancers of half of patients in a clinical trial have progressed
OS: Patients who remain alive from the time of surgery
mOS: The median time at which half of patients in a clinical trial are still alive
New Information from ASCO
Information from ASCO is Encouraging, But Not Conclusive
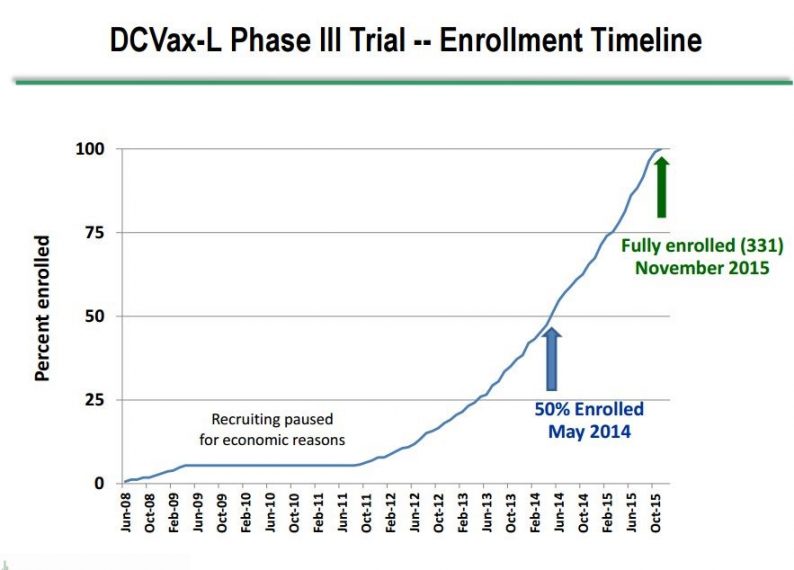
Dr. Marnix Bosch, Chief Technical Officer of Northwest Biotherapeutics, gave a presentation at ASCO on June 5th that provided new information on the phase 3 trial of DCVax-L in patients with newly diagnosed GBM. In his presentation, he showed for the first time a graph of patient enrollment in the trial which indicated that the median time of enrollment was May, 2014, slightly over 3 years ago. This is a very long running trial in which the first patient was enrolled in June 2008 and the last in November 2015. This enrollment timeline is shown below:

Key investigators in the phase 3, DCVax-L trial have stated that patients appear to be living longer than would be expected if they had been treated only with SOC. An encouraging sign of longer patient survival is that the trial was anticipated to end some months ago, but it remains ongoing because the rate of deaths has been slower than expected. The new blinded data released at ASCO further strengthens the hypothesis that we are seeing longer patient survival in the trial due to DCVax—L. Here is what we learned from Dr. Bosch at ASCO.
The median time of enrollment in this 331 patient trial was May 2014, which was 37 months ago as of June. It is important to understand that enrollment in the trial usually starts about three months (actually 13 weeks) after surgery. This means that for patients still alive the length of survival is equal to the time from when they were enrolled plus three months. Keep this three month difference between enrollment and survival in mind.
The first patient was enrolled in June 2008 and the last in November 2015.
There are 100 patients still alive in the trial.
90% of patients in the trial received DCVax-L. Two thirds of the 331 patients were initially given DCVax-L. It is very important to understand that the trial was constructed so that anyone whose cancer progressed then would be given DCVax-L. This meant that patients who progressed on SOC would be switched to DCVax-L and those who progressed on DCVax-L would continue on DCVax-L. This feature allowed the trial to remain blinded, but in actuality, it was close to being a single arm trial.
The reason for keeping patients on DCVax-L after they have progressed is that we have seen in trials of other immune therapies that meaningful survival benefits have been seen in patients even after their cancer progressed.
There are two separate and independent endpoints for the trial-PFS and OS. The minimum stopping threshold for PFS is 248 progression events and that has been reached although Dr. Bosch mentioned in his presentation that further analyses will also be done as part of completing the trial. . The minimum stopping threshold for OS is 233 deaths and as of the ASCO presentation only 231 deaths have occurred. The death rate has slowed to about 2 per month so that the 233 event rate could be reached in July. Importantly, the trial is not likely to be stopped then, but more on this later.
Some Thoughts on the 100 Patients Still Alive
Using assumptions as explained below, I estimate that only 22 of these 100 patients would be expected to be alive if they had received only SOC. It is highly likely that 78 of these 100 patients have experienced a survival benefit due to DCVax-L. It is also important to understand that this does not mean that only these 78 patients benefitted from DCVax-L. As I explain shortly, it is quite probable that some of the other 231 patients who have since died experienced a significant survival benefit before dying. There is just no way to attempt to measure this using information currently available. Here are the assumptions that I used to reach the estimates just cited.
We won’t know precisely how many of these 100 patients were on DCVax-L until the trial is unblinded. However, it seems pretty reasonable to assume that about 90% were on DCVax-L during the trial consistent with the percentage for all 331 patients enrolled. This is essentially a single arm trial with results driven by DCVax-L.
We know that the very last person enrolled in the trial was enrolled 19 months ago so that if this person is still alive and part of the 100 they have survived 22 months since surgery. All other patients in this group of 100 would have survived longer than this.
It would be extremely helpful to know when all of the patients were enrolled and when they died. We could then calculate the length of survival for each and compare to the expected survival if they had been treated with SOC, but this can only be determined when the trial is unblinded. Barring this, maybe we can find a reasonable estimate of the range of survival for the 100. We know that the lower end of the range is 22 months of survival but what is a good estimate of the upper end?
Let me suggest an artificial but still reasonable way of approximating the upper end of the range. Let’s make a simplifying assumption that all 165 or so patients who were enrolled before the median enrollment data of May 2014 have died. This would mean that all of the 100 patients still alive were enrolled between May of 2014 and November of 2015. With this assumption, as of June the survival range would be 22 to 40 months for this group of 100 patients. To the extent that some of these patients were enrolled before May 2014, the 40 month estimate for the upper end of the range would be low.
Clinical trial data suggests that about 36% of GBM patients treated with SOC would be alive at 22 months after surgery and about 8% would survive for 40 months. If these 100 patients had been treated with SOC and if we assume a standard distribution curve for enrollment we can estimate how many of the 100 patients would be expected to survive if they were treated only with SOC. We can simply average the 36% expected survival at 22 months with 8% at 40 months and estimate that about 22% of these 100 patients would be alive. This would indicate that only 22 of these 100 patients would be expected to be alive if they had received only SOC. If so, DCVax-L has provided a survival benefit to 78 of these 100 patients over and above SOC.











Leave A Comment